


The origins of both anger and aggression can be identified in the first years of life. Anger is a primary emotion that emerges in the months after birth (e.g., Lewis, Alessandri, & Sullivan, Reference Lewis, Alessandri and Sullivan1990; Lorber, Del Vecchio, & Slep, Reference Lorber, Del Vecchio and Slep2015; Stenberg, Campos, & Emde, Reference Stenberg, Campos and Emde1983), a few months before infants begin to direct physical force against other people (Eckerman, Whatley, & Kutz, Reference Eckerman, Whatley and Kutz1975). Temper tantrums peak in the second and third years (Potegal & Davidson, Reference Potegal and Davidson2003), around the time that children with problematic levels of aggression begin to be identified (Côté, Vaillancourt, LeBlanc, Nagin, & Tremblay, Reference Côté, Vaillancourt, LeBlanc, Nagin and Tremblay2006). However, is a young child's expression of anger likely to be accompanied by aggression? The aim of our paper was to chart the parallel development of anger and the use of physical force against other people and thereby identify the emergence of a pattern of angry aggressiveness over the first 3 years of life that might predict disruptive impulse control and conduct disorders later in childhood.
The concept of angry aggressiveness extends beyond constructs defined primarily in terms of anger and oppositionality, such as “difficult temperament” (Bates, Reference Bates1980) and oppositional defiant disorder, as opposed to aggression, which is defined behaviorally as a symptom of conduct disorder (American Psychiatric Association, 2013). Angry aggressiveness is similar to Hattwick's (Reference Hattwick1936) concept of children's “contentiousness,” which included both displays of anger and physical aggression. However, anger is more common than aggression. Anger is a primary emotion, expressed in species-specific ways. Some developmental theorists see aggression similarly, as a fundamental human tendency that is universal in the early years of life (e.g., Tremblay, Reference Tremblay2010). In contrast, we have hypothesized that, while most infants begin to express anger by the end of the first year, physical aggression is not as common; the literature suggests that it does not occur at high rates and meaningful individual differences are present from the outset (Hay, Reference Hay2016).
It is important to analyze those individual differences and the risk and protective factors that foster or discourage aggression. The aim of our study was to examine continuity and change in displays of anger and the use of physical force from infancy to childhood, using person-centered (as opposed to variable-centered) statistical methods, which focus on categorizing individuals, not just correlating variables (see below). Person-centered methods allowed us to identify subgroups of infants in a community sample who are already on a pathway toward clinically significant problems with anger management and/or physical aggression, as well as those who show little or no anger or aggression. The person-centered analyses also permitted us to identify those children who might show relatively high levels of anger that was not necessarily combined with physical aggression, in contrast to children who were both angry and aggressive.
We evaluated the contribution of known risk factors for childhood disorder (family adversity and mothers’ mental health) and sought evidence for protective factors that might prevent the development of disruptive behavior. In particular, because the experience of parents’ warmth helps reduce children's behavioral problems (e.g., Pasalich, Witkiewitz, McMahon, Pinderhughes, & Conduct Problems Prevention Research Group, Reference Pasalich, Witkiewitz, McMahon and Pinderhughes2016), we tested whether positive parenting would serve as a protective factor, making it less likely that infants would develop clinically significant behavioral problems in childhood. In contrast, we hypothesized that parents’ endorsement of physical punishment would convey additional risk to the child.
The Origins of Anger and Aggression in Infancy
In this study we focus on expressions of anger and physical aggression that are first detected in infancy (e.g., Tremblay, Reference Tremblay, Lahey, Moffitt and Caspi2003), as opposed to relational aggression, covert conduct problems, and callous-unemotional traits, which emerge later in childhood (for a review see Eisner & Malti, Reference Eisner, Malti, Lerner and Lamb2015). Anger emerges early as an emotional response to frustrating situations when the infants’ goals are blocked or their expectations thwarted (Lewis et al., Reference Lewis, Alessandri and Sullivan1990): from an early age infants express anger through facial expressions, increased motor activity, and negative vocalizations. Despite anger being a primary emotion, individual differences in the proneness to anger are evident in infancy (e.g., Lorber et al., Reference Lorber, Del Vecchio and Slep2015), and a large longitudinal study indicated that atypical patterns of elevated anger at an early age predicted behavior problems in preschool (Brooker et al., Reference Brooker, Buss, Lemery-Chalfant, Aksan, Davidson and Goldsmith2014).
Physically aggressive behaviors develop during the early years (Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004). Individuals differ substantially, not only in the absolute levels of physical aggression they show at a given age, but also in their patterns of aggression over time (e.g., Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007; Côte et al., Reference Côté, Vaillancourt, LeBlanc, Nagin and Tremblay2006; NICHD Early Child Care Research Network, 2004); a finite number of developmental pathways can describe individual differences in aggressive behavior (Broidy et al., Reference Broidy, Nagin, Tremblay, Bates, Brame, Dodge and Pettit2003; Nagin & Tremblay, Reference Nagin and Tremblay2005). Some children may never show aggression; others do so at moderate levels; and some show relatively high levels of aggression that accelerate over time (e.g., Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004).
Individual differences in aggression become evident as soon as infants develop the motor abilities necessary to use force against others. For example, approximately 10% of 12-month-olds within a Dutch community sample displayed oppositional, aggressive, and overactive behavior (van Zeijl et al., Reference van Zeijl, Mesman, Stolk, Alink, van IJzendoorn, Bakermans-Kranenburg and Koot2007). In a Canadian sample, parents’ retrospective reports indicated increasing prevalence in the use of physical force against others (e.g., pushing) between 7 and 17 months of age, with fewer than 5% of infants reported to use force at 7 months, in contrast to 80% by 17 months (Tremblay et al., Reference Tremblay, Japel, Perusse, McDuff, Boivin, Zoccolillo and Montplaisir1999). Infants’ use of force is correlated with other signs of anger and defiance; for example, in a high-risk sample of the children of aggressive parents, infants’ anger, physical aggression, defiance, and activity levels consolidated into a single underlying externalizing dimension, which displayed considerable continuity from 8 to 24 months (Lorber et al., Reference Lorber, Del Vecchio and Slep2015).
The available evidence suggests that, at least for some infants, higher levels of anger may cluster in consistent ways with the use of force against others. In this paper we refer to angry aggressiveness to indicate a pattern of behavior where children's manifest expression of anger is accompanied by the use of force against other people, as reported by parents and other individuals who observe the child in different contexts and situations.
Our previous work in a British community sample using variable-centered methods identified individual differences in angry aggressiveness by 6 months of age (Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010). In that study, because anger and aggression are influenced by context (e.g., Anderson & Bushman Reference Anderson and Bushman2002; Arsenio & Lemerise, Reference Arsenio and Lemerise2004), we collected information from informants who could draw on experiences with the child in different situations and therefore provide a more reliable assessment of the child's behavior (cf. Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006). Individual differences in angry aggressiveness were stable over time. Informants’ reports were validated by direct observation: informants’ ratings of angry aggressiveness were significantly correlated with infants’ distress when confined in a car seat and their observed use of physical force against peers (Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010). Angry aggressiveness in infancy was correlated with well-known risk factors for conduct disorder (Hay, Mundy, et al., Reference Hay, Mundy, Carta, Roberts, Carta, Waters and van Goozen2011) and predicted aggressive conduct problems in early childhood (Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014) and the children's aggressive choices in a computer game 7 years later (Hay et al., Reference Hay, Johansen, Daly, Hashmi, Robinson, Collishaw and van Goozen2017).
Studies of the early origins of aggression, conducted in different laboratories and different countries, reveal stable individual differences across the first 2 years of life. However, the developmental course of aggression shows change as well as continuity. Some children show escalating behavior and develop increasingly severe conduct problems; others eventually desist from the use of force. Although the use of force tends to rise and fall from infancy to early childhood (Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006), that general trend obscures individual trajectories. For example, in one sample, those toddlers who displayed frequent aggressive behavior at 17 months became less aggressive by 29 months (Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007). In another sample, discontinuity in early externalizing behavior was apparent between 8 and 15 months of age (Lorber et al., Reference Lorber, Del Vecchio and Slep2015). The aim of our study was to chart such individual trajectories in angry aggressiveness over time in relation to both risk and protective factors.
Risk and Protective Factors
Risk and protective factors in the family environment influence whether infants become more or less angry and aggressive over time. Responsive caregivers in stable environments are likely to use consistent socialization strategies that help angry infants reduce their use of aggression. In contrast, toddlers who grow up in a less predictable and stable environment may learn that aggressive behaviors are an effective way to pursue their aims when there is no guarantee that these may be satisfied in the future.
Family adversity
Some sociodemographic risk factors that promote children's aggressive behavioral problems are active before birth or in the early months of life (e.g., Pawlby, Hay, Sharp, Waters, & Pariante, Reference Pawlby, Hay, Sharp, Waters and Pariante2011; Pickles et al., Reference Pickles, Hill, Breen, Quinn, Abbott, Jones and Sharp2013; van Goozen, Fairchild, Snoek, & Harold, Reference van Goozen, Fairchild, Snoek and Harold2007). In particular, sociodemographic adversity can affect the development of the child during gestation by exposing the fetus to maternal stress, which increases the risk of developing aggression and other behavioral problems (Robinson et al., Reference Robinson, Mattes, Oddy, Pennell, van Eekelen, McLean and Newnham2011). Exposure to family adversity may increase risk for behavioral problems indirectly, for example, by contributing to economic deprivation that may, in turn, reduce learning opportunities for the child. Sociodemographic adversity may also increase family stress, which in turn may have detrimental effects on family relationships and ultimately on the child's cognitive and socioemotional development (NICHD Early Child Care Research Network, 2004).
Mothers’ mental health
Maternal mental health problems during pregnancy also contribute to children's behavior problems. In particular, stress and depression during pregnancy increases the likelihood of aggression and conduct problems (e.g., Barker, Jaffee, Uher, & Maughan, Reference Barker, Jaffee, Uher and Maughan2011; Hay, Pawlby, Waters, Perra, & Sharp, Reference Hay, Pawlby, Waters, Perra and Sharp2010; Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014; Mäki et al., Reference Mäki, Veijola, Rasanen, Joukamaa, Valonen, Jokelainen and Isohanni2003). The link between prenatal exposure to mothers’ stress and conduct problems is significant even when, due to the use of reproductive technologies, parents are not genetically related to their offspring (Rice et al., Reference Rice, Harold, Boivin, Hay, van den Bree and Thapar2009).
Parents’ attitudes and caregiving practices
It is important to move beyond the foregoing analyses of sociodemographic and psychiatric risk factors to examine the contribution of parents’ attitudes and behavior toward their infants. The effect of parents’ own antisocial behavior may be partly accounted for by the transmission of genetic risk. However, parents with a history of antisocial behavior may also adopt less effective caregiving practices, which in turn may further increase the risk for their children (e.g., Jaffee, Belsky, Harrington, Caspi, & Moffitt, Reference Jaffee, Belsky, Harrington, Caspi and Moffitt2006).
If infants become increasingly prone to anger and resort to using physical force, the way in which their parents and other caregivers react becomes crucial (Belsky, Woodworth, & Crnic, Reference Belsky, Woodworth and Crnic1996; Buck & Dix, Reference Buck and Dix2014; Shaw, Gilliom, Ingoldsby, & Nagin, Reference Shaw, Gilliom, Ingoldsby and Nagin2003). In accordance with Gottfredson and Hirschi's coercion theory (Reference Gottfredson and Hirschi1990), many studies have shown harsh parental discipline to be a risk factor that promotes children's later aggression (Côté et al., Reference Côté, Vaillancourt, LeBlanc, Nagin and Tremblay2006; Shaw et al., Reference Shaw, Gilliom, Ingoldsby and Nagin2003, Shaw, Lacourse, & Nagin, Reference Shaw, Lacourse and Nagin2005; Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004). Parents’ harsh and hostile behavior while attempting to discipline their children often generates conflict and thereby strengthens children's aggressive behavior (Belsky et al., Reference Belsky, Woodworth and Crnic1996). Furthermore, parents’ use of harsh punishment provides a model for physical aggression (NICHD Early Child Care Research Network, 2004), which their children may later emulate.
The study of the role of parental discipline is complicated by societal attitudes and the perceived social desirability of this form of discipline. The use of physical punishment may be difficult to observe when caregivers are aware of being observed; they may be more willing to reveal their attitudes toward the use of harsh discipline when they complete questionnaires designed to control for social desirability effects. Parents' attitudes and beliefs are associated with their caregiving practices (e.g., Socolar & Stein, Reference Socolar and Stein1995). Furthermore, caregivers’ endorsement of harsh discipline predicts their children's externalizing problems in childhood (e.g., Miner & Clarke-Stewart, Reference Miner and Clarke-Stewart2008). Therefore, in the present study, we examined the effect of parents’ endorsement of physical punishment as a risk factor for their children's angry aggressiveness over time.
In contrast, positive parenting, which includes emotional warmth and responsiveness to children's needs, may lower levels of aggression (NICHD Early Child Care Research Network, 2004; Reuben et al., Reference Reuben, Shaw, Neiderhiser, Natsuaki, Reiss and Leve2016). Positive parenting provides a scaffolding family environment, which helps toddlers manage and regulate their own emotions, thus reducing anger and aggressive behavior (NICHD Early Child Care Research Network, 2004). Furthermore, positive caregiving fosters children's own positive social behavior (Boeldt et al., Reference Boeldt, Rhee, DiLalla, Mullineaux, Schulz-Heik, Corley and Hewitt2012), for example, by modeling effective ways to negotiate and manage conflict (Eisenberg et al., Reference Eisenberg, Valiente, Spinrad, Cumberland, Liew, Reiser and Losoya2009). In one study of children who had displayed problematic behavior, mothers’ positive attitudes toward parenting (e.g., their beliefs in praising their children) led to fewer behavioral problems (Denham et al., Reference Denham, Workman, Cole, Weissbrod, Kendziora and Zahn-Waxler2000). In that study, the positive influence of parental attitudes was similar to the effects of their observed behavior. Therefore, parents’ broader attitudes as well as their directly observed positive parenting might exert a combined effect on the development of angry aggressiveness.
Gender differences
In childhood, boys are more likely than girls to show clinically significant neurodevelopmental problems, including oppositional defiant disorder (ODD) and conduct disorder (CD; Maughan, Rowe, Messer, Goodman, & Meltzer, Reference Maughan, Rowe, Messer, Goodman and Meltzer2004). However, these gender differences only gradually emerge over the second and third years of life (Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006; Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007; Hay, Nash, et al., Reference Hay, Nash, Caplan, Swartzentruber, Ishikawa and Vespo2011). In the first year, when the capacity for anger and the use of force is first developing, there is little evidence of gender differences. For example, a meta-analysis of the temperament literature showed that boys were not more likely than girls to show negative emotionality, although infant girls did show higher levels of self-regulation (Else-Quest, Shibley Hyde, Goldsmith, & Van Hulle, Reference Else-Quest, Shibley Hyde, Goldsmith and Van Hulle2006). Studies of the early origins of aggression have not found gender differences in the first year of life (Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006; Hay, Nash, et al., Reference Hay, Nash, Caplan, Swartzentruber, Ishikawa and Vespo2011; Lorber et al., Reference Lorber, Del Vecchio and Slep2015).
Over the next 2 years, when toddlers throw tantrums and learn how to kick or use their fists, parents and other caregivers apply gender-differentiated socialization practices (e.g., Fagot & Hagen, Reference Fagot and Hagan1985). For example, parents respond to boys’ physical aggression in more assertive and directive ways, but when girls are aggressive, they use persuasion and requests to understand the victim's perspective (Smetana, Reference Smetana1989). Gender-differentiated socialization contributes to the increasing divergence between boys and girls. Therefore, when identifying different trajectories toward angry aggressiveness, it is important to test for gender differences.
The Value of Person-Centered Statistical Analyses
The literature on the early development of aggression has mainly focused on individual differences in the “level” of behavior. Aggressive behavior is often thought of as a single underlying dimension that varies quantitatively across individuals. However, development entails qualitative as well as quantitative change. Infants and toddlers’ developing motor and cognitive abilities influence not only the level of their aggressiveness but also the organization of its emotional and behavioral elements. New behaviors emerge over time. For some infants, an early propensity to express anger may eventually translate into acts of physical force. Other infants who were initially similar in their levels of anger may be much less likely to resort to physical aggression. Therefore, longitudinal analyses of the development of aggression must focus on qualitative changes in anger and the use of force over time, in relation to risk and protective factors.
In this study, we used person-centered analyses to identify subgroups of infants who showed qualitatively different developmental patterns over time. Person-centered statistical methods identify homogenous groups of individuals within a sample, defined by shared characteristics (e.g., von Eye & Bergmann, Reference von Eye and Bergmann2003). In our study, two types of person-centered analyses—latent class and latent transition analyses—were used to track groups of infants with qualitatively different patterns of angry aggressiveness across the first 3 years of life, thus identifying those individuals in the sample who were most likely to escalate or de-escalate over time. We hypothesized that infants who showed either angry aggressiveness at consistently high levels or a pattern of escalation over time would be at elevated risk for clinically significant disorder later in childhood.
Such use of person-centered longitudinal methods to identify high-risk subgroups in infancy is relevant for prevention and intervention research, and ultimately for clinical practice. If well-characterized high-risk groups can be identified in the first year of life, effective prevention strategies might begin in infancy, before the high-risk children are already manifesting serious symptoms of disruptive behavior disorders (McMahon & Frick, Reference McMahon, Frick, Prinstein, Youngstrom, Mash and Barkley2019). By revealing patterns of individual difference, person-centered methods also address the common assumption that all infants are naturally aggressive.
Specific Aims
In sum, our specific aims were to (a) identify subgroups of infants who show different levels and configurations of angry aggressiveness over time; (b) investigate continuity and discontinuity in development by analyzing how subgroup membership might change or remain stable from infancy to early childhood; (c) investigate changes in subgroup membership in relation to gender and family risk factors; (d) test for the differential impact of parents’ attitudes and behavior that reflect positive parenting as opposed to the endorsement of physical punishment; (e) determine whether those infants with high or escalating levels of angry aggressiveness were at elevated risk for aggressive conduct problems at age 3 years; and (f) predict from angry aggressiveness group membership in infancy to clinical diagnoses of CD and/or ODD with impairment at age 7 years.
We anticipated a degree of discontinuity across development, including patterns consistent with the concept of “multifinality” (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996), which acknowledges that infants who start out similar might diverge over time. In line with earlier evidence, we hypothesized that boys and girls would display increasingly divergent patterns over time. We hypothesized that positive parenting would be protective whereas parents’ endorsement of harsh discipline would increase the risk for children's angry aggressiveness.
Method
Design
The Cardiff Child Development Study (CCDS) is a six-wave prospective longitudinal study of the social and emotional development of a nationally representative community sample of firstborn children whose mothers were recruited from antenatal clinics in two Healthcare Trusts in South Wales. Mothers and, where possible, fathers were interviewed during the last trimester of pregnancy. The children were assessed at mean ages of 6, 12, 21, 36, and 84 months (7 years), respectively, in an alternating sequence of home and laboratory visits.
Participants
Families in which the mother was expecting her firstborn child had been recruited in pregnancy through UK National Health Service prenatal services; 332 families participated in pregnancy, with 321 (97%) remaining in the sample after the child was born. No exclusion criteria were set other than the infant's death, or illness so serious that the infant could not be assessed. The present paper focuses on a subsample of 304 infants (173 boys) for whom there was information on at least one anger or aggression questionnaire item provided by at least one informant, on at least one measurement occasion between infancy and early childhood; this subsample represented 92% of the original 332 families who had been recruited during pregnancy.
Demographic characteristics of the 304 families included in the subsample for this paper are presented in Table 1. The CCDS sample was found to be nationally representative as shown by analyses that compared family demographic characteristics of the CCDS sample with the subsample of firstborn children in the Millennium Cohort Study, the most recent national birth cohort study in the United Kingdom (K. Kiernan, personal communication, April 2009). Procedures were approved by the Cardiff University School of Psychology Research Ethics Committee and the UK National Health Service Multi-Centre Research Ethics Committee.
Table 1. Maternal characteristics before birth of the child, and parenting attitudes and behavior when the child was 6 months

aRetrospective self-report measure collected during last pregnancy trimester. bSelf-report measure collected around infancy visit. cObserved behavior during 6-month visit. dConstruct estimated with a measurement model with the positive behaviors during the infancy visit as indicators.
Procedure
Pregnancy
During pregnancy, two interviewers visited the participants’ homes, administering questionnaires and conducting separate interviews with the mother and, if possible, the other parent (99% biological fathers; 1% same-sex partners). Both parents provided information in 80% of families (94% of couples in committed relationships).
Infancy
A total of N = 301 families (91% of those recruited in pregnancy) participated in a second home visit with a target age range of 5 to 7 months (M = 6.64 months, SD = 0.88, range 5–11), with 9 other families providing questionnaire data only. Parent–infant interactions were observed across three tasks, each 3 min in duration: a free play task in which the parent was asked to play a familiar game; a joint activity task in which the parent was asked to show the infant an activity board with flaps like a book; and a feeding task in which the parent was asked to feed solid food to the infant (or water if the infant was not yet eating solid food). Questionnaires were completed by mothers, fathers, and a third family member or friend who knew the infant well.
To enable the comparison of the parents’ observed behavior with their attitudes, we focused on the infants’ primary caregivers, with N = 295 (280 mothers and 15 fathers) observed in the interaction tasks (5 families have missing data due to technical difficulties with the video and one child could not participate in the tasks due to developmental delay). A total of N = 258 primary caregivers (248 mothers and 10 fathers) completed the parenting questionnaires. Multiple imputation methods were used to deal with missing information on observed and self-reported parenting behavior (see Data Analysis section).
At a mean of 12 months, families were invited to the university to take part in laboratory-based assessments; a brief questionnaire was completed by the family member (90% mothers) who accompanied the infant to the laboratory. Because multiple informants did not report on the infant's behavior at that time, those data are not included in the longitudinal analyses for the present paper.
Toddlerhood
Another home visit with a target age range of 18 to 24 months took place at a mean age of 20.63 months (SD = 2.26, range 17 to 30 months). Questionnaires were again completed by mothers, fathers, and a third family member or friend (N = 258 families).
Early childhood
Families were invited to take part in a laboratory visit within a target range of 30 to 42 months. In N = 254 families, questionnaires were again completed by mothers, fathers, and a third family member or friend at a mean age of 36.12 months (SD = 7.18, range 27 to 66 months).
Middle childhood
The final assessments in the study were carried out within a target age range of 6 to 7 years during two home visits. A total of N = 287 children participated at a mean age of 83.28 months (SD = 4.54, range 67 to 104 months). Questionnaires were completed by mothers, fathers, and classroom teachers. The primary caregiver (97% mothers) was interviewed about the family environment and the child's mental health, using a semistructured clinical interview.
Measures
Family adversity
Because many of the indicators of sociodemographic adversity were highly intercorrelated, a general index of child's exposure to maternal factors known to be associated with overall family adversity was created using principal component analysis (PCA). Maternal reports of sociodemographic variables were used for each family, in order to equate the source of information across the different family structures found in this community sample of first-time mothers and infants. These family structures encompassed single mothers and mothers in a relationship with a partner who was not the biological father of the child (including same-sex partners), as well as mothers who were in a committed relationship with the child's biological father. A series of items endorsed by mothers during prenatal interviews and questionnaires contributed to the adversity index:
(a) Occupational status, assessed using the Standard Occupational Classification 2000 (SOC2000; Elias, McKnight, & Kinshott, Reference Elias, McKnight and Kinshott1999), is a recommended criterion used to measure social class in British cohorts. The highest ranked employment the mother ever had was used to determine her occupational status. If she had never been in paid employment, the highest ranked occupation in her household was used to estimate her social class. Mothers’ scores on the SOC2000 scale were dichotomized into the working class and middle/upper class as defined by the SOC2000 criteria.
(b) Maternal education, described by a dichotomous variable indicating whether the mother had failed to attain the basic level of educational qualifications expected in the United Kingdom: at least five General Certificate of Secondary Education examinations passed at Grades A* to C or, for older members of the sample, the equivalent Certificate of Secondary Education or “O”-level grades.
(c) Mother not being in a committed romantic relationship during the pregnancy, defined as not living with or otherwise having a romantic commitment to the child's biological father.
(d) Mother not being legally married during the pregnancy.
(e) Young maternal age, dichotomized according to whether or not mothers were younger than 20 years of age at the time of the child's birth.
A PCA based on the polychoric correlation matrix confirmed that all these categorical items contributed to a single component, with eigenvalues 3.84 and 0.68 for the first and second component extracted, respectively. The first component explained approximately 77% of the shared variance in these risk indicators. Summary scores derived from the PCA were used in all subsequent analyses as an index for family adversity.
Maternal prenatal depression
The mood disorder and anxiety sections of the Schedules for Clinical Assessment in Neuropsychiatry (Wing et al., Reference Wing, Babor, Brugha, Burke, Cooper, Giel and Sartorius1990) were incorporated into the prenatal interviews. Interviewers had received formal training. Independent coding was carried out using DSM-IV criteria, while final decisions concerning clinical diagnosis were made in conferences with two experienced psychiatrists and a trainee clinical psychologist. Significant interrater agreement was reached between the clinicians’ diagnoses of disorder, κ = .78, p < .001. A random sample (20%) of participants who did not meet caseness criteria was also assessed by two clinicians, confirming that disorder was not present. DSM-IV mood disorder was categorized into major depressive disorder or bipolar disorder. Mothers were classed as depressed in pregnancy if they had been diagnosed with major depressive disorder or bipolar disorder with predominantly depressive features in that time period. The interview was repeated at the early infant home visit and diagnoses made in the same way, with good reliability, κ = .80, p < .001.
Mothers’ antisocial behavior
During the prenatal interviews, mothers reported on their history of arrest and symptoms of antisocial personality disorder, using the screening questionnaire for the International Personality Disorder Examination (Loranger et al., Reference Loranger, Sartorius, Andreoli, Berger, Buchheim, Channabasavanna and Regier1994) combined with seven items measuring DSM-IV symptoms of CD. The resulting composite measure of mothers’ past and present antisocial behavior showed good internal consistency (Cronbach's α = .79) and was further validated by mothers’ reports of their history of arrest, r (323) = .56, p < .001.
However, preliminary analyses indicated that the inclusion of mothers’ antisocial behavior and antenatal depression as covariates caused problems of model convergence. On closer inspection, these problems seemed to be related to the association between these two variables (Spearman's ρ = .31, p < .001) and problems related to lack of common support (see Murnane & Willett, Reference Murnane and Willett2011), that is, the fact that associations between exposures to risk factors and outcomes cannot be reliably estimated when few participants are present in different regions of the covariates’ cross-tabulation (e.g., when only a few mothers who were depressed before birth did not also display antisocial tendencies). To avoid this problem, the measure of mothers’ antisocial behavior was dichotomized at the median. Although this resulted in a potential decrease of power to detect associations between outcomes and mothers’ antisocial behavior, we reasoned that dichotomizing this variable would result in a more stringent test of the associations, which was preferable than the alternative when considering estimates biased by lack of common support.
Parenting attitudes and behavior
At a mean of 6 months postpartum, the parents’ attitudes about childrearing were assessed via the Parental Attitudes toward Childrearing Questionnaire (PACQ; Easterbrooks & Goldberg, Reference Easterbrooks and Goldberg1984), which includes six items that tap into parents’ beliefs in warm parenting (comforting, showing affection, praising, joking and playing, providing attention, and feeling satisfaction in being a parent, α = .69). The composite PACQ warm parenting variable was asymmetric and skewed, and therefore was power-transformed for further analyses. Means, standard deviations, and range of raw scores on this measure are reported in Table 1.
The PACQ also contained two items measuring the parents’ endorsement of physical punishment, which were combined (Table 1). This variable was also asymmetric and therefore was log-transformed in further analyses.
During the home observation at the infancy visit, the primary caregiver's observed positive affect (smiling and laughing) was coded using 10-s interval time sampling across the three interactive tasks. Independent observers recorded 34% of the videos with good agreement (median intraclass correlation = .96). A measurement model was constructed that considered the cumulative instances of smiling and laughing displayed by the primary caregiver in the three interaction tasks as indicators. Because the indicators were count variables, the estimator used in the measurement model was the maximum likelihood estimator with robust standard errors in Mplus 7 (Muthén & Muthén, Reference Muthén and Muthén2012). The model indicated a good fit, LR χ 2 (972) = 683.4, p = 1.00. The positive affect scores derived by this measurement model (see Table 1) displayed a distribution approaching normality.
Angry aggressiveness from infancy to early childhood
At the infancy, toddlerhood, and early childhood visits, up to three informants rated the child's anger and aggressive behavior using the Cardiff Infant Contentiousness Scale (CICS). This instrument, whose name draws on Hattwick's (Reference Hattwick1936) pioneering work on children's angry aggressiveness, uses age-appropriate items that measure anger and use of physical force, which were embedded into a checklist of normative developmental milestones (e.g., smiles; can sit up by himself/herself; see Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010). The infant form of the CICS administered at the infancy visit contains four age-appropriate items: infants’ angry moods, temper tantrums, biting others, and hitting out at others (e.g., moving their arms to strike another person). Two further age-appropriate items were included in the toddler form of the CICS at the toddler and early childhood visits in order to take into account toddlers’ motor development: hitting or kicking to get toys and forcefully grabbing toys or objects from others.
Informants reported on the occurrence of these behaviors in three ordered categories of response (does not occur; sometimes/possibly occurs; often/definitely occurs). The four- and the six-item scales have internal consistency, significant inter-rater agreement, and concurrent and predictive validity (for details see Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010; Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014).
CICS data from the infancy visit were available for 287 infants; in 61% of cases, all three informants provided data; in 15%, only one informant provided data. At the toddler visit, CICS data were available for 258 children, with all three informants providing information for 67% and only a single informant in 11%. At the early childhood visit, CICS data were available for 244 children, with information provided by all three informants in 62% of families and by only one informant in 18%.
The analytic approach used in subsequent analyses requires a focus on individual items from the CICS infant and toddler scales. We obtained a cross-informant composite score for each CICS item by averaging scores across informants at each age and categorizing these scores in three brackets (coded 0, 1, and 2), using as cut points scores of 0.65 and 1.65 to round the average score up to the next category.
CICS questionnaires were available across all three ages for 212 infants (70%), while 61 (20%) had information on at least two occasions. Analyses of missing data patterns revealed that at each age missingness was significantly and positively associated with higher levels of sociodemographic adversity, but not with prenatal depression or mothers’ antisocial behavior. We concluded that missingness was predicted by variables other than the outcome of interest and therefore data were overall missing at random, that is, missing in ways that are associated and can be predicted by covariates. Therefore, cases with missing scores on different occasions were still included in subsequent analyses. By adopting full information maximum likelihood, latent class models use all available information in the estimation of model parameters. This feature ensures that parameters are estimated more reliably compared to an analysis that only uses complete cases; as long as the reasons for missing data are stochastic (missing completely at random) or dependent on covariates included in the analysis (missing at random), the full information maximum likelihood method provides unbiased estimates.
Children's aggressive conduct problems in early childhood
At the early childhood visit, 254 families reported on the child's clinically significant behavioral and emotional problems using the 1.5- to 5-year-old version of the Child Behavior Check List (CBCL; Achenbach & Rescorla, Reference Achenbach and Rescorla1992). The CBCL aggressive problems scale yields an age-appropriate continuous measure of young children's aggressiveness and associated conduct problems. Mothers’ ratings on the aggressive problems scale were significantly correlated with fathers’ ratings, r (168) = .46, p < .001, and with ratings provided by the third informant, r (172) = .49, p < .001. A factor score was derived considering all available information provided by up to three informants using a measurement model; mothers’, fathers’, and third informants’ ratings were considered indicators of a latent dimensional construct. These factor scores, analogous to standardized scores, were constrained to have a mean of 0 and SD = 1. Mplus 7 (Muthén & Muthén, Reference Muthén and Muthén2012) was used to implement this measurement model and calculate factor scores. A maximum likelihood estimator with robust standard errors was used to allow for nonnormal distributions of the indicators.
Children's mental health at the middle childhood visit
At the middle childhood visit, the child's primary caregiver was interviewed using the Preschool Age Psychiatric Assessment (PAPA; Egger et al., Reference Egger, Erkanli, Keeler, Potts, Walter and Angold2006), which covers the full range of behaviors that are symptoms of psychopathological disorders of children under the age of 8 years. Interviewers were trained by an official PAPA trainer and monitored throughout the data collection period. The data were sent to Duke University for independent analysis, using SAS algorithms designed to identify cases of DSM-IV disorders with clinical impairment. The PAPA has been used to estimate prevalence of CD and ODD in prior studies of epidemiological samples (e.g., Wichstrøm et al., Reference Wichstrøm, Berg-Nielsen, Angold, Egger, Solheim and Sveen2012). In the present sample, 12% of children met the DSM-IV criteria for CD and/or ODD with significant clinical impairment. Although the PAPA algorithms were based on DSM-IV criteria, we note that the joint focus on CD and ODD is compatible with the approach now taken to identifying these phenomena within the broader category of disruptive, impulse-control, and CD in DSM-5.
Data analysis
Person-centered analyses were used to investigate individual differences and sequences of change over time in configurations of children's anger and aggressiveness. These methods permit identification of different subgroups of infants who differ in their patterns of anger and use of force. Latent transition analysis (LTA), as opposed to mixture growth models, was used because LTA allowed for the investigation of qualitative changes, particularly changes that might produce newly emerging configurations of angry aggressiveness (Flaherty, Reference Flaherty2008). The use of LTA also permitted a focus on patterns of discontinuity across ages (Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007), that is, identifying children who move from one configuration of angry aggressiveness to a different configuration as they grow older.
Data preparation was conducted using Stata 13 (StataCorp, 2013). Latent class and latent transition analyses used Mplus 7 (Muthén & Muthén, Reference Muthén and Muthén2012). These analyses were conducted in different stages, following the advice given by Ryoo, Wang, Swearer, Hull, and Shi (Reference Ryoo, Wang, Swearer, Hull and Shi2018). The stages of analysis are numbered to map the analytic stages onto the reported findings.
i. Cross-sectional latent class analysis (LCA) models
Cross-sectional LCA models were tested with an increasing number of classes to ascertain the best latent class solution that could describe the different configurations of angry aggressiveness at the infancy, toddlerhood, and early childhood assessments. We assessed the best latent class solutions using the Bayesian information criteria (BIC) and the sample-sized adjusted BIC (a-BIC) to compare different models: lower values indicate better fit. Indicators of the quality of classification such as entropy (McCutcheon, Reference McCutcheon, Hagenaars and McCutcheon2002) were also considered, as reported in the online-only Supplementary materials.
ii. Tests for longitudinal measurement invariance
Next, we tested for measurement invariance in the latent class solutions estimated at the different time points, which allowed investigation of the consistency of the latent constructs being assessed, that is, the different categories of anger and aggressiveness. This step informed the longitudinal measurement model used in subsequent investigations of change across time.
iii. LTA with risk factors as covariates
In the next stage of analysis, the longitudinal measurement model identified in (ii) was used to test for changes in angry aggressiveness across age. LTA is an autoregressive model whereby the current status (e.g., high levels of angry aggressiveness) is determined by the individual's status on a previous measurement occasion. This effectively means that an individual's current status at Time 2 is expressed as a function of the probability of transitioning into that status, given the individual's status at previous Time 1.
At this stage of analysis, risk factors were introduced as covariates, which allowed us to determine how gender and family risk factors (family adversity, mothers’ prenatal depression, and mothers’ history of antisocial behavior) were associated with infants’ anger and use of force in infancy. Latent categories in toddlerhood and early childhood were then regressed on the same covariates while controlling for the latent status at the previous age. In this way we tested whether these risk factors influenced transitions across age from one latent category to another.
iv. LTA with parents’ warmth and endorsement of harsh punishment as covariates, adjusting for other covariates
At the fourth stage of analysis, we tested whether different transition patterns from infancy to toddlerhood, and from toddlerhood to early childhood were associated with positive parenting and/or endorsement of harsh punishment, as measured in infancy. The parents’ endorsement of punishment and the positive parenting variables significantly and negatively correlated; in order to avoid collinearity, we introduced these two groups of variables in separate regressions. To this purpose, parents’ endorsement of punishment was entered as a covariate in the model described in the third analytic stage (iii). Next, in a further regression, parents’ endorsement of warm parenting and observed positive affect during parent–infant interaction were entered into the covariates introduced in stage iii, thus assessing the adjusted associations between these parenting variables and transition patterns in angry aggressiveness. To allow for missing information in the parenting variables, these analyses were conducted on 50 imputed data sets created using multiple imputation chained equations (Stata 13 command mi: StataCorp, 2013). Auxiliary variables used to increase prediction accuracy included the angry aggressive latent class affiliation in infancy, toddlerhood, and early childhood; prenatal depression; mother's depression during the infant's first 6 months; the family adversity index; and mother's history of antisocial behavior. The latent transition models in Mplus thus averaged parameters across the 50 imputed data sets provided by N = 304 (i.e., those participants with any information about angry aggressiveness, as described above).
v. LTA to predict aggressive conduct problems in early childhood
To investigate whether participants’ configurations of anger and aggressiveness from infancy to early childhood predicted aggressive conduct problems at age 3 years, we tested whether infants’ anger and aggressiveness status in infancy and toddlerhood predicted their symptoms on the CBCL aggressive scale in early childhood. In order to avoid bias due to missing data in the CBCL scores, missing CBCL scores were imputed in 50 complete data sets using chained equation in Stata 13 (StataCorp, 2013). Auxiliary variables used to increase prediction accuracy included the angry–aggressive category membership in infancy, toddlerhood, and early childhood; family adversity; mothers’ prenatal depression; and mothers’ history of antisocial behavior.
vi. LTA in relation to the distal outcomes of CD/ODD with clinical impairment in middle childhood
At the final stage of analysis, we tested whether a child's configuration of angry aggressive behavior in the first years of life predicted whether or not that child met DSM-IV criteria for a diagnosis of CD or ODD in middle childhood. The latter analyses were conducted by running logistic regression models in Stata 13 (StataCorp, 2013); the latent class affiliation estimated in infancy, toddlerhood, and early childhood by the latent transition models was considered one of the predictors of the outcome, while controlling for other covariates: family adversity index, mothers’ history of antisocial behavior, and the child's gender (preliminary checks had shown that prenatal depression was not related to the outcome). In conducting these regressions, we controlled for the uncertainty in assigning children to latent classes by using weights that represented children's probability of being in each one of the latent classes estimated at a given age (the probability weighting methods described in Clarke & Muthén, Reference Clarke and Muthén2009). Furthermore, because of missing data in the follow-up outcomes of interest, we estimated regression parameters from 50 complete data sets created using multiple imputation methods that use chained equations: these are implemented in the mi command of Stata13. Auxiliary variables used to increase prediction accuracy of the outcomes included the angry–aggressive latent class affiliation in infancy, toddlerhood, and early childhood; the family adversity index; and mother's history of antisocial behavior. The results represent averaged parameters across the 50 imputed data sets provided by N = 304 participants with information about angry aggressiveness.
Results
Descriptive statistics
The average frequency of informants’ responses to the angry aggressive items at each age are reported in the online-only Supplementary material. Table 1 reports key statistics concerning the risk factors considered. Some of these risk factors were intercorrelated: the family adversity index was significantly related to mothers’ antisocial behavior and prenatal depression, r (332) = .40, p < .0001 and r (332) = .44, p < .0001, respectively, but was not significantly associated with the child's gender, r (329) = .10, p = .07. Mothers’ prenatal depression was significantly correlated with the dichotomized measure of mothers’ antisocial behavior, ρ (332) = .47, p < .0001. Although the association between prenatal depression and the gender of the baby was nonsignificant, ρ (329) = –.05, p = .65, the association between mothers’ history of antisocial behavior and having a male child was significant, ρ (329) = .20, p = .02.
The findings regarding parents’ positive parenting are drawn from the self-reported and directly observed data provided by the primary caregiver (mother or father) who was present for the interaction tasks. Parents’ endorsement of physical punishment was negatively correlated with their beliefs in warm parenting, r (256) = –.17, p = .005. Parents’ observed positive affect, as measured by the dimension derived across the three observational tasks, was positively associated with their beliefs in warm parenting, r (247) = .14, p = .03, and was negatively related to their endorsement of physical punishment, r (245) = –.13, p = .04.
Aim 1: Identifying subgroups of infants with different levels and configurations of anger and aggressiveness over time
Data analysis Step i: Cross-sectional LCA
In infancy and early childhood, the best solution explaining variability in angry aggressiveness was a three-ordered-class solution. In ordered classes (McCutcheon, Reference McCutcheon, Hagenaars and McCutcheon2002), the probability of informants who reported that the infant showed a behavior increased from one class to another. In contrast, in toddlerhood, the best solution was a four-ordered-class solution, followed by one with three ordered classes. However, closer inspection revealed that the fourth class included fewer than 10 participants, who were categorized in the highly angry–aggressive group in the three-ordered-class solution but manifested even more extreme levels of behavior than other toddlers in that subgroup. This extreme group was not large enough and sufficiently distinct in its features to be considered further; therefore, the three-ordered-class solution was retained as the final model for all ages.
The three subgroups of children showed qualitative as well as quantitative differences between them. A relatively small group of participants at each age displayed high levels of physical force as well as emotional displays of anger (see Figure 1). We have thus dubbed this group “high anger–high aggression” (HH). A second group displayed elevated levels of anger, but in contrast to the former one, this group only showed moderate levels of physical force directed at others. This group was dubbed “high anger–moderate aggression” (HM). Finally, a third group of participants displayed lower levels of angry aggressiveness: this was dubbed the “low anger–low aggression” (LL) group. The percentages of infants in the HH, HM, and LL classes at each age are shown in Figure 2.

Figure 1. Conditional probabilities of endorsing CICS items by the three latent class groups in infancy, toddlerhood and early childhood. Conditional probabilities constrained to be consistent across periods are indicated with an x.
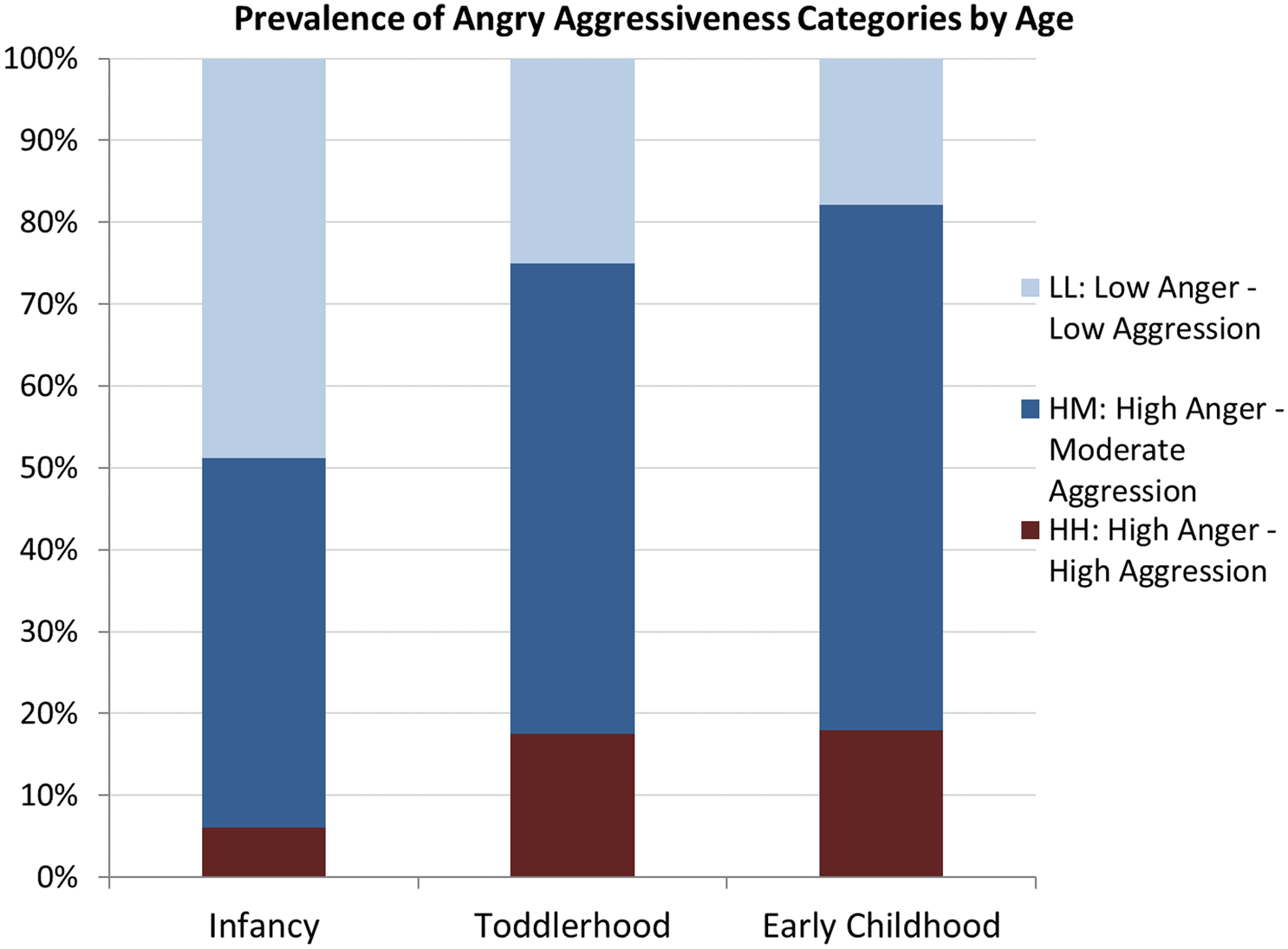
Figure 2. Prevalence of angry aggressiveness categories by age.
Aim 2: To investigate continuity and discontinuity in angry aggressiveness by analyzing how groups might change or remain stable from infancy to early childhood
Data analysis Step ii: Tests for longitudinal measurement invariance
In LCA, measurement invariance places constraints on the probability of endorsing an item, conditional on latent class membership. We tested different measurement models before imposing autoregressive relations between the latent categorical variables (following recommendations by Nylund, Reference Nylund2007) and using likelihood ratio tests (LRT) between nested models to test the fit.
A full-invariance model provides a strong assumption of invariance, with each conditional probability of an item constrained to be the same across measurement occasions. However, this highly constrained model did not provide an acceptable fit, as indicated by a worsening of model fit compared to a model with no measurement constraints, LRT χ2 (34) = 154, p < .001; therefore, the full-invariance model was rejected.
A partial-invariance model assuming invariance of indicators across the classes was then tested. Based on inspection of conditional probabilities in unconstrained models, the partial-invariance model assumed invariance for all items within the HH subgroup with the exception of the item angry moods. Furthermore, the frequency of angry moods, hitting out at others, kicking/hitting to obtain toys, and grabbing toys was also invariant across age for the HM subgroup. Finally, the frequency of hitting was invariant across ages for the LL subgroup. These constraints are highlighted in Figure 1.
This partial measurement invariance model displayed an acceptable fit compared to the unconstrained noninvariance model, LRT χ2 (25) = 29.81, p = .23, as well as lower BIC and a-BIC values, respectively, those being 5955.3 and 5739.6 for the noninvariance model versus 5860.8 and 5724.4 for the partial-invariance model. The HH group was less invariant than the other groups, showing general consistency in its measurement parameters across age. The HM group showed invariance in key indicator behaviors such as anger, hitting, and kicking. The LL class was the most variant class across age, with different behaviors showing different probability from age to age. In sum, with respect to Aim 2, there was some continuity in the categories underlying angry aggressive behavior from infancy to early childhood, insofar as an invariant category of children who displayed high anger and high aggression (HH) and a relatively stable category characterized by high anger but moderate aggression (HM) were consistently identified. The category characterized by lower levels of angry aggressiveness (LL) was somewhat less consistent across age (see Figure 1).
Aim 3: To investigate the contribution of the child's gender and family risk factors in predicting changes in subgroup membership over time
Associations between variables
Before summarizing the results of the LTA with covariates, we first report the associations between the family risk factors and the child's gender and the latent classes identified at each time point (Table 2). There were several significant associations between the latent classes and these predictors. In particular, the maternal risk factors (prenatal depression and history of antisocial behavior) were associated with children's angry aggressiveness status in infancy, toddlerhood, and early childhood. A strong association was observed between angry aggressiveness status in infancy and family adversity, whereby infants in the HH category displayed higher adversity scores. A nonsignificant trend was observed between gender and angry aggressiveness in infancy, but these variables were significantly associated in early childhood, when boys displayed a higher prevalence of HM angry aggressiveness compared to girls.
Table 2. Descriptive associations between family and child variables and by latent class (LC) status and by age

Note: HH, high anger–high aggression. HM, high anger–moderate aggression. LL, low anger–low aggression.
Data analysis Step iii: LTA with maternal risk factors as covariates
The model with partial measurement invariance from infancy to early childhood was taken forward to investigate continuity and transitions from one category to another across age. The child's angry–aggressive status at one age was regressed on his or her angry–aggressive status at the previous age, while controlling for covariates.
In the estimated model, the percentage of HH infants increased from infancy to toddlerhood and then remained stable from toddlerhood to early childhood. Fewer than half of the infants fell into the HM angry–aggressiveness category in infancy, but subsequently the majority of the sample fell into this category. In infancy, nearly half the infants (49%) had shown little or no anger or use of force, but fewer fell into the LL category in toddlerhood and early childhood.
The transition probabilities of moving from one category to another are reported in Table 3. Despite the general rise in angry aggressiveness from infancy to toddlerhood, some degree of continuity in membership over time was revealed: over half of all infants remained in the same subgroup as toddlers and 65% of children remained in the same subgroup from toddlerhood to early childhood. Those infants who were highly angry and aggressive (HH) at 6 months never fell to the LL group in toddlerhood, and only 7% of the sample showed such an extreme decrease between toddlerhood and early childhood. Transitions from the neither angry nor aggressive group (LL) to the highly angry–aggressive category (HH) were also infrequent. With age, there was an increase from LL to HM levels of angry aggressiveness (see Figure 2). In sum, there was some degree of stability in individual differences across age, against the background of a general increase in anger and use of force between infancy and toddlerhood.

Figure 3. Means and 95% Confidence Intervals on the CBCL aggression scale for the three latent class groups in infancy, toddlerhood, and early childhood.
Table 3. Probabilities of transitioning from one angry–aggressive class to another across age

Note: HH, high anger–high aggression. HM, high anger–moderate aggression. LL, low anger–low aggression.
Stability probabilities (i.e., probability of remaining in the same class across two adjacent measurement points) are shaded.
The parameters of the multinomial regressions describing the adjusted associations between risk factors and the categories of angry aggressiveness are reported in Table 4. In what follows we examine these associations in more detail.
Table 4. Odds ratios (OR) and 95% CI (confidence intervals) of being in the high anger–high aggression (HH) and high anger–moderate aggression (HM) angry–aggressive categories compared to the low anger–low aggression (LL) category by age, N=304. ORs in toddlerhood and early childhood are adjusted controlling for angry aggressiveness status in the previous measurement occasion. In this way, the ORs represent changes in the odds of transitioning into an angry–aggressiveness category rather than the reference one (LL).

+p < .06. *p < .05. **p < .01.
Gender differences
Although more boys were in the HH and HM categories in infancy (see Table 2), gender differences were not significant when controlling for other covariates, as reported in Table 4. However, the analyses for change over time revealed that gender differences became apparent in the patterns of change between toddlerhood and early childhood. Boys were more likely than girls to move from the LL group to the HM group in early childhood (odds ratio [OR] = 3.57; 95% confidence interval; CI [1.00, 12.72]).
Family risk factors
Family adversity as measured before the child's birth was strongly associated with the infants’ initial levels of anger and their use of force in infancy (see Table 4). After controlling for other covariates, a 1 SD increase in the infant's level of exposure to adversity was associated with a threefold increase in the likelihood of being in the HH rather than the LL subgroup (OR = 3.12; 95% CI [1.00, 9.76]) and with a twofold increase in the odds of being in the HM rather than the LL subgroup (OR = 2.09; 95% CI [1.35, 3.24]).
We then tested for associations between these risk factors and angry aggressiveness at later ages, while controlling for the infant's angry aggressiveness category at the previous age. The multinomial logistic regression parameters revealed a significant association between mothers’ antisocial behavior and infants’ moderate angry aggressiveness (HM) in toddlerhood: after controlling for other covariates and the infant's level of angry aggressiveness at 6 months, mothers’ antisocial behavior was associated with a twofold increase in the odds of moving to the HM rather than the LL group (OR = 2.56; 95% CI [1.03, 6.31]).
Those infants whose mothers had been depressed during pregnancy displayed increased odds of transitioning into the highly angry–aggressive (HH) class (3.28, 2.76, and 1.24 in infancy, toddlerhood, and early childhood, respectively, but these associations were not reliable due to the large confidence intervals.
In sum, the family adversity index was significantly associated with initial differences in infants’ anger and use of force at the earliest age studied, while the mother's own history of antisocial behavior was associated with escalating patterns in her child's angry aggressiveness between infancy and toddlerhood, with boys in particular showing escalation from toddlerhood to early childhood (see Table 4). No significant associations between prenatal depression and children's patterns of angry aggressiveness were found.
Aim 4: Test for the differential impact of parents’ positive parenting as opposed to the endorsement of harsh discipline
Associations between variables
Table 5 reports the association between latent class affiliation and the parenting variables measured in infancy, as well as the fit of multinomial regressions of latent class affiliation on each of these variables. Parents’ beliefs in warm parenting showed a gradient across the three angry–aggressive categories at the toddler visit, with the parents of highly angry and aggressive toddlers (HH) less likely to endorse warm parenting and parents of the least angry and aggressive infants (LL) reporting stronger beliefs in warm parenting; these differences approached significance (Table 5). The parents’ expressed positive affect during the interaction tasks was unrelated to the infants’ initial level of angry aggressiveness at 6 months; however, the parents’ positive affect at 6 months significantly predicted the configurations of angry aggressiveness in toddlerhood and early childhood (Table 5). No significant associations between parents’ endorsement of physical punishment at 6 months and their children's level of anger and aggressiveness were observed at any time point.
Table 5. Means and SD of parenting variables measured in infancy by latent class (LC) status and by age. Parenting variables were regressed on the nominal latent class affiliation with summary statistics reported.

Note: HH, high anger–high aggression. HM, high anger–moderate aggression. LL, low anger–low aggression. +p < .06. *p < .05.
Data analysis Step iv: LTA with parents’ warmth and endorsement of harsh punishment as covariates, adjusting for other covariates
Multiple imputation was used to account for missing parenting variables, with parameters of analyses averaged across 50 complete data sets. The key results are reported in Table 6.
Table 6. Adjusted odds ratios (OR) and standard errors (SE) of being in the high anger–high aggression (HH) and high anger–moderate aggression (HM) angry–aggressive categories compared to the low anger–low aggression (LL) category, by parenting variables and by age, N = 304. ORs in toddlerhood and early childhood are adjusted controlling for angry aggressiveness status in the previous measurement occasion. In this way, the ORs represent changes in the odds of transitioning into an angry–aggressiveness category rather than the reference one (LL).

Note: Parameters are estimated across 50 completed data sets created using multiple imputation. When estimating parameters based on multiple imputations, Mplus does not estimate 95% confidence intervals. Here we report the SE of the ORs. The models controlled for associations between latent classes and other covariates (child gender, family adversity, prenatal depression, and maternal history of conduct problems). *p < .05. **p < .01. ***p < .001.
Parents’ endorsement of punishment
In an initial regression, we considered parents’ endorsement of punishment as a covariate, while controlling for other covariates. As the preliminary analyses had suggested, the parent's endorsement of punishment was not associated with the child's anger and use of force in infancy or with successive transitions (results reported in the online-only Supplementary Material).
Parents’ observed positive affect and belief in warm parenting
A second regression included the parent's observed positive affect and belief in warm parenting as predictors of the child's angry aggressiveness (Table 6). After controlling for the child's angry aggressiveness status, infants whose parents reported stronger beliefs in warm parenting had decreased odds of moving from the LL class into the HH class between the infancy and toddler assessments (OR = 0.48), and significantly reduced odds of moving from the LL class to the HM class (OR = 0.56). Thus, the children of parents who held stronger beliefs in warm parenting were less likely to escalate to higher levels of angry aggressiveness over time.
Similarly, those infants who experienced higher levels of parents’ positive affect during the interaction tasks at the infancy visit were less likely to escalate in their angry aggressiveness between toddlerhood and early childhood; a 1 SD increase in parent's observed positive affect in infancy was associated with a 68% reduction in the odds of moving to the HH rather than the LL category between toddlerhood and early childhood, OR = 0.32. Similarly, a 1 SD increase in parents’ positive affect during the interaction tasks was associated with a 66% decrease in the odds of moving to the HM rather than the LL category between toddlerhood and early childhood, OR = 0.34 (see Table 6). In sum, parents’ beliefs in warm parenting and observed positive affect while interacting with their infants were associated with de-escalating patterns of angry aggressiveness.
Aim 5: To test whether infants with high or escalating levels of angry aggressiveness were at elevated risk for aggressive conduct problems at age 3 years
Data analysis Step v: LTA to predict aggressive conduct problems in early childhood
An unconditional latent transition model was used to assess associations between angry aggressiveness categories in infancy and toddlerhood and the CBCL aggression scale factor scores in early childhood (M = 36 months). Overall, 254 infants who were included in the latent transitions analyses had been assessed by one or more informants (mother, father, or other family member) using the CBCL aggression scale.
Figure 3 displays the means and 95% CI of the CBCL aggression scale by latent class affiliation in infancy, toddlerhood, and early childhood. Separate multiple regressions examined the latent class affiliation at mean ages of 6 and 21 months as predictors of the CBCL aggression scores. Parameter estimates were weighted by individuals’ probability of being in a given angry–aggressiveness subgroup at each age, respectively, thus controlling for uncertainty in estimated latent class affiliation (Clark & Muthén, Reference Clarke and Muthén2009). The regression models also controlled for risk factors (child's gender, family adversity, mothers’ prenatal depression, and mothers’ history of antisocial behavior). Analyses were conducted averaging parameters across 50 complete data sets created using chained equations.
Prediction from infancy
The findings revealed a significant association between angry–aggressive status in infancy and CBCL aggression scale scores in early childhood, F (6, 288.4) = 3.61, p < .01. After controlling for other covariates, those infants in the HM category, as contrasted with infants in the HH category, had significantly lower CBCL aggression scale scores (coefficient = –0.45, SE = 0.21, t = –2.16, p = .032), as did those infants who had shown the lowest levels of angry aggressiveness at 6 months (coefficient = –0.70, SE = 0.21, t = –3.25, p < .001).
Prediction from toddlerhood
Latent class status in toddlerhood also significantly predicted CBCL aggression scores in early childhood, F (6, 287.5) = 6.93, p < 001. Compared to the HH group in toddlerhood, those in the HM group had lower CBCL aggression scores (coefficient = –0.56, SE = 0.13, t = –4.36, p < .001), as did those who had shown little or no anger or aggression in toddlerhood (coefficient = –0.85, SE = 0.15, t = –5.72, p < .001).
In sum, the findings demonstrated predictive associations, whereby infants showing the highest levels of anger and use of force in infancy were reported to have the greatest number of aggressive conduct problems by 3 years of age.

Figure 4. Odds ratios and 95% Confidence Intervals of childhood CD and/or ODD for the HM and HH latent class groups in infancy, toddlerhood and early childhood, adjusting for covariates. The LL group was the reference group: Odds ratios indicated changes in the odds of childhood CD/ODD for participants in the HM or HH group compared to those in the LL group.
Aim 6: To test whether infants with high and/or escalating levels of angry aggressiveness were at elevated risk for clinical diagnoses of CD and/or ODD in middle childhood
Data analysis Step vi: LTA to predict the distal outcome of CD/ODD with clinical impairment in middle childhood
When the PAPA interview was administered at a mean age of 7 years, 33 (12%) of the children met criteria for CD or ODD with clinically significant impairment. Two-way crosstabulations revealed associations between the angry aggressiveness subgroups in infancy and toddlerhood and diagnoses of CD/ODD in childhood. Of note, about a quarter (25%) of those in the HH group in infancy, toddlerhood, and middle childhood met diagnostic criteria for CD/ODD with clinical impairment at 7 years of age (Table 7).
Table 7. Number and percentages of participants in angry–aggressive classes at each time point who met criteria for CD/ODD at 7 years.

Note: HH, high anger–high aggression. HM, high anger–moderate aggression. LL, low anger–low aggression. CD, conduct disorder. ODD, oppositional defiant disorder.
Associations between angry–aggressive categories in the first 3 years and diagnoses of CD/ODD at age 7 persisted after controlling for covariates (gender, family adversity, and mothers’ history of antisocial behavior) in logistic regression models (see Figure 4). Analyses were conducted on an imputed complete data set to avoid bias due to incomplete data.
Prediction from infancy to diagnosis
A marginal association was observed between angry–aggressive categories in infancy and CD/ODD at 7 years (Figure 4). Compared to infants in the LL group in infancy, those in the HM subgroup displayed a twofold increase in the odds of meeting diagnostic criteria for CD/ODD at 7 years (OR = 2.42, 95% CI [0.95, 6.13], t = 1.86, p = .06).
Prediction from toddlerhood to diagnosis
A significant association was observed between angry–aggressive categories in toddlerhood and CD/ODD at 7 years. Compared to those in the LL category, toddlers in the HH group displayed over a fourfold increase in the odds of meeting diagnostic criteria for CD/ODD at 7 years of age (OR = 4.75, 95% CI [1.16, 19.51], t = 2.16, p = .03).
Prediction from early childhood to diagnosis
A marginal association was also observed between being in the HH group in early childhood and CD/ODD at 7 years. Compared to those in the LL category, those toddlers categorized as highly angry–aggressive displayed a nearly eightfold increase in the odds of meeting criteria for CD/ODD (OR = 7.94, 95% CI [0.91, 69.48], t = 1.87, p = .06). In sum, the results indicated a pattern of associations between early levels of anger and aggressiveness and risk for CD/ODD at 7 years (see Table 6 and Figure 4).
Discussion
The findings of these person-centered analyses of a representative longitudinal sample confirm earlier evidence for significant individual differences in anger and the use of force in infancy (Côte et al., Reference Côté, Vaillancourt, LeBlanc, Nagin and Tremblay2006; NICHD Early Child Care Research Network, 2004; Lorber et al., Reference Lorber, Del Vecchio and Slep2015), and have corroborated and extended the prior variable-centered analyses on our sample (Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010; Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014). In terms of the theoretical debates about the developmental origins of aggression, the new evidence from person-centered analyses provides further support for our hypothesis that individual differences in the display of anger and the use of physical force are already present in the first year of life (Hay, Reference Hay2016). Our findings provide information on the clustering across early stages of development of anger and the use of force against other people, lending support to our conceptualization of angry aggressiveness as children's proneness to displays of anger combined with physical aggression.
Our findings extend existing evidence by (a) identifying particular subgroups of infants at different levels of risk for problematic aggression; (b) demonstrating patterns of change and discontinuity over time that showed either escalation or de-escalation from earlier levels of angry aggressiveness; (c) providing evidence for both risk and protective factors that influence the pattern of change over time and risk for later conduct problems; and (d) providing evidence that very high levels of angry aggressiveness in infancy and toddlerhood are relatively uncommon and may herald the development of clinically significant oppositionality and conduct problems later in childhood.
Identification of subgroups of infants at differential risk
We used LCA and LTA to chart changes in angry aggressiveness from early infancy to age 3 years. These methods permitted detection of emerging behavior patterns, beyond merely quantitative changes in the frequency of particular behaviors across development (Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007; Connell et al., Reference Connell, Bullock, Dishion, Shaw, Wilson and Gardner2008). The identification of three ordered groups by LTA may initially suggest an underlying dimensionality of angry aggressive behavior. However, closer inspection of these categories revealed important qualitative as well as quantitative differences that influenced the pattern of change in angry aggressiveness over the first 3 years. Crucially, these categories indicated differences in the range of behaviors shown: To emphasize these qualitative differences, we have dubbed the groups that showed higher levels of angry aggressiveness high anger–high aggression (HH), and high anger–moderate aggression (HM). While infants and toddlers in the HH and HM angry aggressiveness category were both prone to angry outbursts, they diverged in their use of physical force (Figure 1). Compared to the HH subgroup, individuals in the HM subgroup seemed better able to avoid translating their anger into physical aggression.
Not all infants were angry or aggressive. At all ages, some children showed very low levels of both anger and aggression: this group was dubbed low anger–low aggression (LL). However, over time, most children in the sample were reported to show higher levels of anger, with the size of the HM subgroup increasing from infancy to toddlerhood. Thus, across the toddler years, displays of anger become more normative but physical force continued to be used more sparingly in both the HM and the LL group. It is noteworthy that the most common form of physical force for the HM group was a form of instrumental aggression, grabbing of toys; in contrast, the HH group were more likely to direct force against other people's bodies.
Again, it is important to note that these subgroups could reliably be identified by 6 months of age. Previous investigators have suggested that in infancy there would be individual differences in proneness to anger, but only at a later stage would that anger be expressed through physical aggression (Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006; Tremblay, Reference Tremblay, Lahey, Moffitt and Caspi2003). The results of our study do not support this claim. Rather, even at 6 months of age, a minority of infants in the HH group were not only expressing anger but also reported to hit out at or bite others; the informants’ reports were validated by observations of those infants’ directly observed use of force against peers (Hay, Mundy, et al., Reference Hay, Mundy, Carta, Roberts, Carta, Waters and van Goozen2011). The divergence of our findings from received wisdom in the literature is not due to sample discrepancies: the rates of highly angry aggressive toddlers in our community sample resemble the rates of highly aggressive children identified in larger surveys of aggression (e.g., Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004).
Consistency and change in subgroup membership over time
Overall, although many children remained in the same category across measurement points, some change did occur, which corroborates earlier findings (Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007; Lorber et al., Reference Lorber, Del Vecchio and Slep2015). The proportion of infants classified as high in angry aggressiveness (HH) increased over time, an increase that was primarily accounted for by infants in the high anger–moderate aggression (HM) group who moved into the HH category by the time of the toddler visit. This shift in subgroup membership over time may partly reflect the well-established increases in temper tantrums (Potegal & Davidson, Reference Potegal and Davidson2003), possibly because children's developing locomotor skills increase opportunities for frustration and conflict with family members (Campos, Kermoian, & Zumbahlen, Reference Campos, Kermoian and Zumbahlen1992). Some changes in angry aggressive behavior occur during the transition from infancy to toddlerhood (e.g., Lorber et al., Reference Lorber, Del Vecchio and Slep2015).
Nevertheless, despite normative increases in the occurrence of tantrums and development of the motor abilities needed to deploy force against other people, those infants in the LL group who showed the lowest levels of angry aggressiveness did not move into the HH group at later ages. Some change occurred in the opposite direction, with some HH infants moving down to the HM category; however, those infants in the HH group never moved all the way down to the LL group. Rather, HH infants remained at elevated risk for aggressive conduct problems at 36 months.
Gender differences
Patterns of change were associated with gender differences; compared to girls, boys were more likely to show escalation from LL to HM angry aggressiveness. However, these gender differences did not emerge until early childhood. This finding corroborates other studies indicating that, while individual differences in anger and use of force are already present in infancy, gender differences emerge gradually over the first 3 years of life (Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006; Baillargeon et al., Reference Baillargeon, Zoccolillo, Keenan, Côté, Pérusse, Wu and Tremblay2007; Hay, Nash, et al., Reference Hay, Nash, Caplan, Swartzentruber, Ishikawa and Vespo2011; Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014). This emerging divergence between girls and boys probably derives from a series of cascading factors (Hay, Reference Hay2016). Some of these are biological, for example, gender differences in maturation rate and males’ higher susceptibility to neurodevelopmental problems (Hay, Reference Hay2007). Others are related to cultural norms and differences in socialization processes, for example, gender-differentiated treatment by parents (e.g., Smetana, Reference Smetana1989).
Some investigators have argued that the biological differences between girls and boys may moderate the relationships between early risk factors and children's problem behavior (e.g., NICHD Early Child Care Research Network, 2004). This issue is further complicated by temperament (e.g., van Zeijl et al., Reference van Zeijl, Mesman, Stolk, Alink, van IJzendoorn, Bakermans-Kranenburg and Koot2007) and emerging differences in self-regulation that drive girls’ and boys’ differential susceptibility to parenting practices (Chang, Olson, Sameroff, & Sexton, Reference Chang, Olson, Sameroff and Sexton2011). For example, in future work, it would be important to explore gender differences in response to positive parenting, which we have here shown to be a protective factor against the escalation of angry aggressiveness.
Although none of these factors alone explain the eventual gender difference, together they produce a cascade of developmental outcomes that lead to the striking differences in later childhood. Emerging gender differences may also be further amplified by young children's preference for same-sex interaction; peers as well as parents may foster gender differences in angry aggressiveness (Hay, Reference Hay2007; Hay, Nash, et al., Reference Hay, Nash, Caplan, Swartzentruber, Ishikawa and Vespo2011).
The influence of family risk factors
Sociodemographic adversity was associated with increased odds of a child being in the HH angry aggressiveness group by 6 months of age, replicating findings from other studies (NICHD Early Child Care Research Network, 2004; Lorber et al., Reference Lorber, Del Vecchio and Slep2015; Shaw et al., Reference Shaw, Lacourse and Nagin2005; Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004; van Zejl et al., Reference van Zeijl, Mesman, Stolk, Alink, van IJzendoorn, Bakermans-Kranenburg and Koot2007). Exposure to adverse family circumstances may contribute to increased risk for problematic behavior in different ways. Some mechanisms may be more direct: adversity (e.g., economic hardship, low educational attainment, and lack of social support) may raise pregnant women's levels of stress, which in turn may interfere with the development of infants’ stress response systems (van Goozen et al., Reference van Goozen, Fairchild, Snoek and Harold2007). Adversity may increase stress for the whole family, thus contributing to social environments and caregiving practices that amplify propensities for dysregulated and disruptive behavior (NICHD Early Child Care Research Network, 2004). Our findings suggest that exposure to social adversity predicted interindividual differences that were already evident at a very early age.
In our sample, other risk factors were associated with escalation of angry aggressiveness from infancy to toddlerhood. In particular, the mothers’ own history of antisocial behavior predicted infants’ escalation from LL to HM levels of angry aggressiveness. Genetic influence and gene–environment interplay may contribute to the observed link between parents’ antisocial behavior and escalation of angry aggressiveness. It would be useful to test for such influences in genetically informative designs.
Positive parenting as a protective factor against the escalation of aggression
Our findings also draw attention to the importance of parents’ beliefs in positive parenting and their expression of enjoyment while interacting with their infants, which complements earlier findings of a link between difficulties in the mother–infant relationship and infants’ early anger and aggressiveness (Lorber et al., Reference Lorber, Del Vecchio and Slep2015). Positive parenting protected against the escalation of angry aggressiveness from infancy to childhood; parents’ beliefs in warm parenting promoted de-escalating patterns of angry aggressiveness from infancy to early childhood. The parents’ observed smiling and laughing while interacting with their infants similarly predicted de-escalation of angry aggressiveness.
Previous studies have suggested that parents’ influence on the development of aggression may be particularly important in toddlerhood, a time when parents’ responses to toddlers’ frustration and aggression may play a crucial role (Belsky et al., Reference Belsky, Woodworth and Crnic1996; Shaw et al., Reference Shaw, Gilliom, Ingoldsby and Nagin2003). However, our results draw attention to the importance of earlier parent–infant interaction and parents’ attitudes and values that are already established in infancy. Positive interaction between infants and caregivers promotes emotion regulation, which may in turn help infants deal with emotional challenges without showing extreme anger or resorting to physical force (NICHD Early Child Care Research Network, 2004). Parental warmth also supports toddlers’ on-task planning behavior and reduces impulsivity (Reuben et al., Reference Reuben, Shaw, Neiderhiser, Natsuaki, Reiss and Leve2016). Parents’ beliefs in warm parenting may promote positive and supportive interactions between parent and child, even when the child's behavior becomes increasingly more challenging in the toddler years. In future work it would be important to acknowledge the bidirectionality of parent–child relationships and examine children's effects on their parents’ attitudes and expression of emotion, and how that might influence parents’ warmth and parenting strategies over time.
Our findings showed that positive parenting was protective against the escalation of angry aggressiveness across all three subgroups, which has important implications for early prevention strategies. Even those infants who are already showing high levels of angry aggressiveness profit from a warm caregiving environment and positive parental attitudes.
Long-term consequences of early angry aggressiveness
Individual differences in angry aggressiveness in infancy and toddlerhood were predictive of aggressive conduct problems by 3 years of age and clinically significant disruptive, impulse control, and CD by 7 years of age. These findings support our claim that, even in early stages of development, angry aggressiveness represents a coherent behavioral construct, and individual differences in infants’ and toddlers’ expression of angry aggressiveness hold significance for their future development and adaptation to the social world.
Some explanations of the developmental trends we have observed may invoke cumulative effects of risk factors. For example, adverse family circumstances contribute to more unstable family relationships over the course of childhood, which in turn has detrimental effects on the child's emotional and behavior development. It is also possible that early appearing individual differences in angry aggressiveness may contribute to the development of clinically significant problems through a process of “reverse causality”: infants’ and toddlers’ early forms of aggressive behavior may evoke more negative parenting practices (e.g., harsh discipline), in an attempt to control the child's behavior. However, our results showed that early appearing signs of angry aggressiveness led to less adaptive and problematic behavior later in childhood, regardless of the parents’ inclinations to use harsh punishment. In contrast, positive parenting was protective.
Limitations of the study
The analyses presented in this paper rely heavily on informants’ reports of infants’ angry aggressiveness and behavioral problems, and thus some continuity over time may reflect shared methods variance. We tried to address this problem by using multiple informants who observed the infant's behavior in different contexts (see Alink et al., Reference Alink, Mesman, van Zeijl, Stolk, Juffer, Koot and van IJzendoorn2006). There was a higher probability of receiving reports from only one informant when families lived under challenging conditions. However, most infants in the sample were reported on by at least two informants, and the informants’ reports showed good interrater agreement. Furthermore, the ratings of angry aggressiveness across informants were validated at each age by objectively observed measures of infants’ frustration and aggressive interactions with peers (Hay, Perra, et al., Reference Hay, Perra, Hudson, Waters, Mundy, Goodyer and van Goozen2010; Hay et al., Reference Hay, Waters, Perra, Swift, Kairis, Phillips and van Goozen2014).
Although the sample size might also be seen as a limitation, compared to studies of larger populations, recruitment of a sample of moderate size permitted the use of direct observation in naturalistic settings as well as multiple informants. There were relatively low levels of attrition, and the longitudinal analyses reported here used robust statistical procedures, including the use of multiple imputation methods to counter bias due to nonresponse. The categorization of infants into subgroups was not derived through arbitrary cutoff points but rather through statistical probability models.
Implications of the findings
Our longitudinal study allowed us to take an explicitly developmental perspective, using person-centered methods to move beyond earlier variable-centered evidence for continuity of individual differences at the group level to a focus on individual patterns of escalation and de-escalation over time. The person-centered approach provided additional insight into the way in which positive parenting can inhibit the escalation of aggression.
Our findings indicate that, as much as we might like to assume that most toddlers are aggressive and naturally grow out of it, there is considerable benefit in acknowledging that a minority of 1- and 2-year-olds who show very high levels of anger and use of force against other people are already on a pathway toward clinically significant conduct problems. Appreciation of individual variation in early infancy and its consequences for later problems may lead to screening procedures that help identify those infants and parents who are in particular need of support. The encouraging finding that positive parenting can help prevent the escalation of angry aggressiveness from infancy to early childhood provides important evidence that can inform the development of very early prevention strategies to lower a child's risk for serious conduct problems. We have shown that prevention strategies that encourage positive parenting could begin before the first birthday.
Supplementary material
Supplementary material available online at https://doi.org/10.1017/S0954579420000243
Acknowledgments
We thank the other members of the Cardiff Child Development Study team and the participating families who have so generously given their time to this longitudinal study. We are grateful to the anonymous reviewers who have contributed to improving this manuscript thorough their feedback.
Financial support
The Cardiff Child Development Study has been supported by Medical Research Council Programme Grant GO400086 and Medical Research Council Project Grant MR/J013366/1.













